What we talk about when we talk about chronomedicine
I was reading this article on circadian variation in immune response a couple of weeks ago when I came across this quote, seemingly engineered in a lab to get my adrenaline pumping:
“McKeating [says] that when she thinks back to the long line of failed vaccines in this field, she wonders whether timing may have been a key factor that was previously ignored.”
Timing! Not just the time on the wall clock but biological time. Your “circadian state” at the moment of dosing. Of course, that could matter, and if it could matter, why not keep track of it? Why not control for it when you’re trying to understand why your trial succeeded or failed?
When we talk about circadian medicine, or chronomedicine, or chronotherapy, what we’re saying is that the fact that your body changes over the course of the day implies that medicine—treatment efficacy, treatment side-effects—could change too. Not for every drug, not for every target. But with half the genome regulated by the circadian clock, aiming for precision in medicine without thinking about circadian rhythms feels like trying to hit a target with an arrow without thinking about the direction of the wind. Rhythmicity shouldn’t just be an afterthought; it’s the medium of our existence.
Take melatonin, the hormone for night that gets naturally produced once per day in our bodies, as driven by our circadian clock. Melatonin isn’t slightly elevated at some times versus others. It’s absent, and then it’s there. It’s like this:
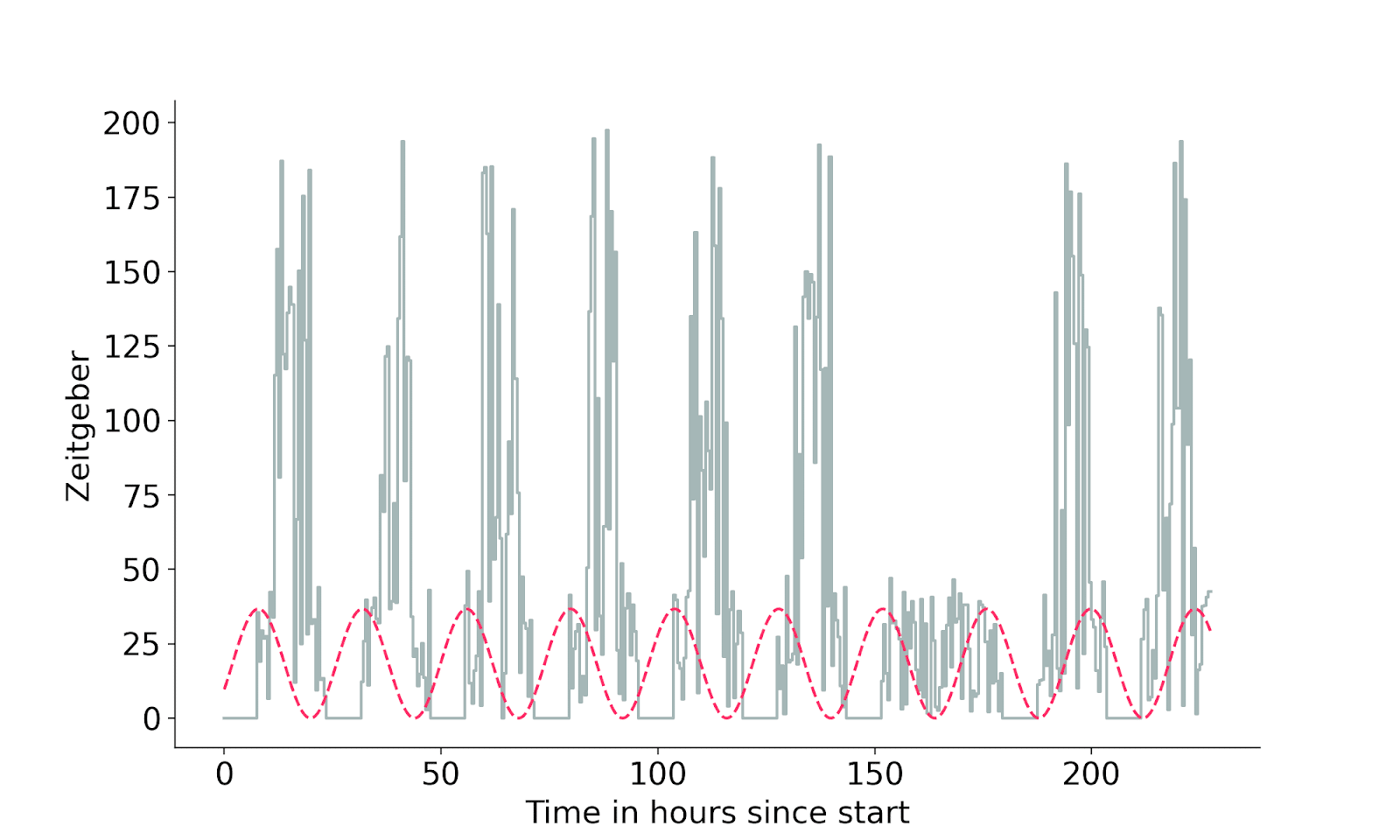
So one way your body changes radically over the day is in how much melatonin is gushing through your bloodstream. This is one way of thinking about “what time your body thinks it is.” Want to know an example of a drug that does different things to you depending on what time your body thinks it is?
(Drum roll, please.)
Melatonin!
Melatonin, as the pill you can buy in the U.S. at a convenience store, is a drug where we actually have a pretty good idea of how it operates if you dose with it at different biological times. In a sense, we know its “efficacy curve.”
There are some times when pill-based melatonin acts to speed up your body’s circadian clock, and there are other times when it does the opposite and slows your body’s clock down. Its efficacy curve looks something like this:
There’s a somewhat funny punchline here which is that it’s possible to take melatonin at a time that should make it harder for you to fall asleep the next day (by way of slowing down/delaying your body’s natural rhythm for sleep). But more than that: if you dosed with melatonin randomly over the course of the day and looked to see what effect it had—namely, how much it sped up or slowed down your clock, in aggregate—you wouldn’t see one. The effect would be washed out because the times it was speeding up your clock would be counteracted by the times it was slowing things down.
Of course, most people aren’t going around taking melatonin during the hours where it slows your body’s clock down. But some people sure are! People who have irregular schedules; people who’ve recently crossed time zones; people who work nights. All of these people are playing “what will melatonin’s effect be” roulette every time they pop a pill because they’re ignoring the importance of circadian time. They’re trying to hit the target but not paying attention to the wind.
There is, of course, a very simple answer to “why not keep track of circadian timing” in clinical trials and research, which is that most experimental measures of circadian time are massively painful to get. Nobody running a clinical trial is going to want to ask participants at scale to come sit in the dark for six to 24 hours spitting into tubes to identify their dim light melatonin onset, the gold standard biomarker for circadian time. Not only does that quickly become logistically infeasible—it’s also prohibitively costly.
Here’s where we come in. Arcascope’s technology removes the need for invasive circadian tests in large scale studies: predicting hidden internal quantities, like when your naturally produced melatonin is going to start to rise, from noninvasive measures, like long-term time series of signals from your phone and wearables.
Let’s start by helping people figure out what melatonin, or light, or a workout is going to do to their body at different times. But let’s get to a place where we don’t have to wonder if timing could have made the difference in a failed trial: making tracking timing in clinical trials and research the standard.